

Safe, Healthy, and Thriving
How culturally safe health care hubs can close the gap for Aboriginal children in care.


The child protection system is not meeting the health needs of Aboriginal children in care. We need to reorient toward a more integrated health and wellbeing framework that is preventative, supportive, strengths based and culturally safe. This urgently requires a national strategy, a commitment to self-determination and building on the strengths of the ACCHO1 model, a robust regulatory and reporting framework, and stronger collaboration between the child protection and health systems. By keeping health and wellbeing at the heart of child protection policy and practice, we have the potential to change the trajectories of children in care.
Aboriginal2 children represent more than one third of children in out-of-home care (OoHC),3 even though they account for only 5.9% of Australia’s children.4 They are more than ten times more likely to be in care than non-Aboriginal children,5 and numbers are rising. Projections from current data suggest that the number of Aboriginal children in care could increase by 54% by 2030.6
The high health care needs of children in OoHC is well documented in international and Australian literature.7,8 Yet in Australia these needs are largely unmet with even the minimum standard of health care recommended in national guidelines due to deep deficiencies in the funding and oversight of health for children in OoHC.For Aboriginal children, these factors are exacerbated in part due to an inequitable access to health care.9 As a result, many Aboriginal chidren in OoHC have undetected health and neurodevelopmental problems10-12 that affect their ability to productively engage in education, employment, and society.
The child who is disruptive in class might have an undiagnosed hearing impairment due to a treatable middle ear disease.
The adolescent who is chronically late to school and always tired might have undiagnosed sleep apnoea and require surgery.
The child who is aggressive and dysregulated may never have had trauma-informed therapy to address the family violence he experienced.
The child who is failing school may have an undiagnosed speech and language disorder, and may never have had speech therapy, or access to an evidence-based literacy program.
Within the paediatric clinic at the Victorian Aboriginal Health Service, where I have worked as a paediatrician for more than eight years, more than half of the Aboriginal patients I see are in OoHC. In this manner, it has functioned as a defacto OoHC clinic despite limited funding to do so. This is because it is seen as a culturally safe service. In contrast, a nearby state-funded multidisciplinary clinic specifically designed for children in OoHC saw just 17 Aboriginal children over three years of operation, according to published data.13 This lack of access to health care comes at a high cost to the lives of children in care, and a social and economic cost to both the Aboriginal and broader Australian community. A report by the Telethon Kids Institute examined the cost of late intervention in Australia, finding that the greatest cost (39%) was attributed to OoHC: around $5.9 billion annually.14 An inquiry found that two-thirds of Aboriginal children in Victoria’s youth justice system had been in OoHC and many more were known to the child protection system.15
The intergenerational impacts are considerable as well. Graduates of the OoHC system are more likely to have their children enter care,16 and are four times more likely to remain on income support payments.17 These trajectories could be changed if we reoriented the child protection system towards strengths-based and culturally safe services that provide integrated health and wellbeing assessments, therapy, and support for children and families.
At a national level, there is a sound framework to achieve this through the detailed health guidelines for children in OoHC, the National Clinical Assessment Framework for Children and Young People in Out-of-home Care (2011)18 (NCAF, Figure 1).

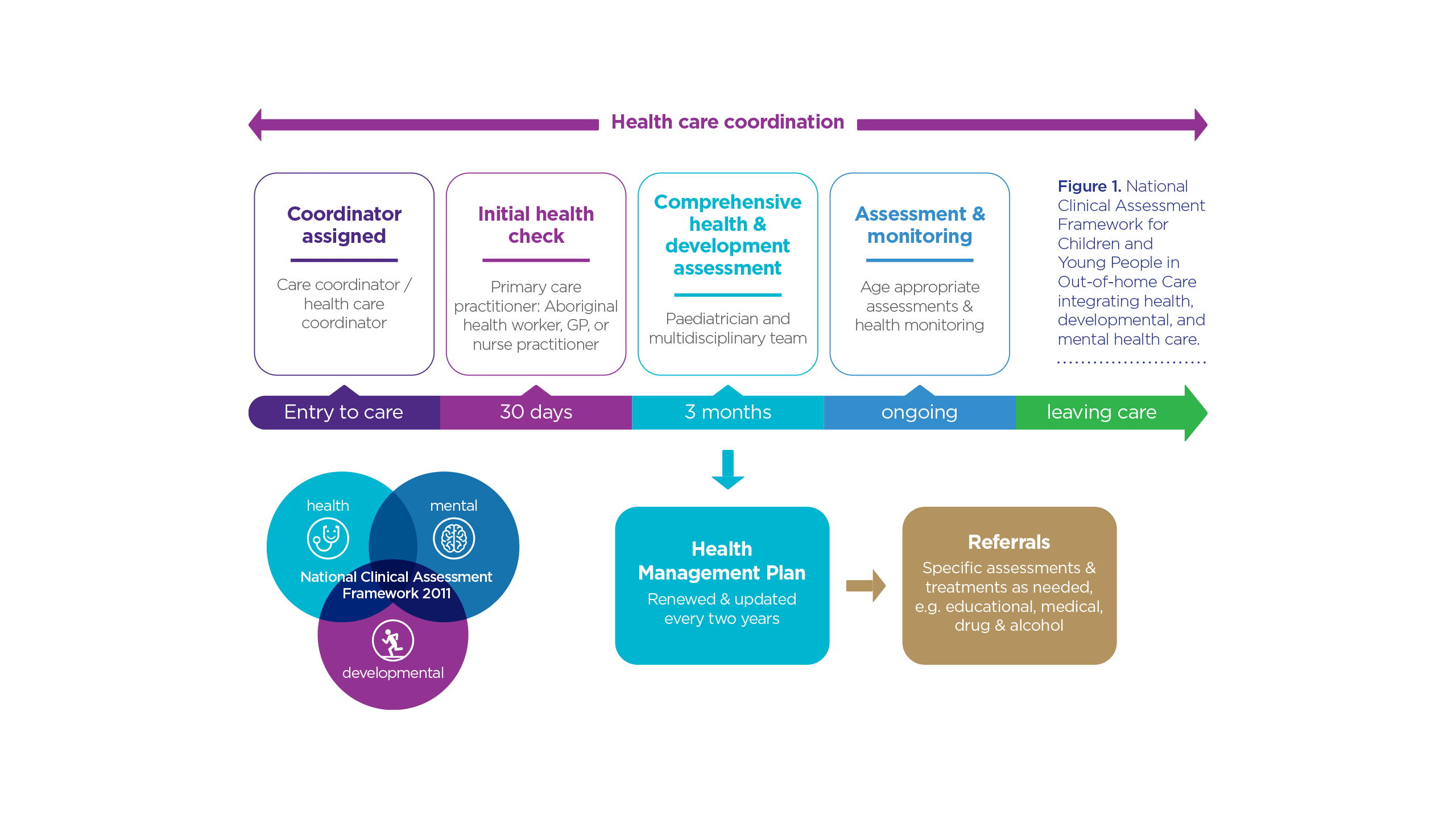
The NCAF recognises the need to develop a standardised system of care in order to detect, intervene, and improve health outcomes for all children in OoHC as part of the National Framework for Protecting Australia’s Children (2009) and National Standards for Out-of-home Care. The NCAF contains detailed evidence-based and age-tiered guidelines for preliminary health checks and comprehensive multidisciplinary assessments led by paediatricians across three health domains: physical, developmental, and psychosocial and mental health. The NCAF recommends the development of health management plans and coordination of care.
The broad aim of the NCAF is to improve the health of children in OoHC, a population known to have high health needs, through the early identification and treatment of health, neurodevelopmental and mental health problems. It is aligned with best practice internationally, and the recommendations of professional medical groups in Australia, including the Royal Australasian College of Physicians19 and the Royal Australian and New Zealand College of Psychiatrists.20
Despite having a solid national health care framework for children in OoHC, a key issue has been the NCAF’s implementation, which to date has been patchy and variable at best. The states and territories hold statutory responsibility for child protection and health,21 and as such, are required to provide state specific services. Yet a recent Victorian study found that less than 1% of the state’s children in OoHC had received all recommended health care in line with the NCAF within a year of entering care.22 This low rate of implementation is due to several factors. At a federal level, the NCAF is not supported by specific Medicare rebates, nor Commonwealth funding. At a sub-national level, most states have limited health infrastructure or capacity to run such specialised services.23 Another issue is oversight. Though Standard 5 of the National Standards for OoHC24 stipulates for health care to be delivered in a timely manner, there is no statutory requirement to comply with the NCAF and subsequently there is poor measurement and reporting of these standards, and little accountability for non-compliance.25
To address the complex needs of children in OoHC, it is crucial to have coordinated, integrated, accessible hubs of health and supportive services. However, with the notable exception of Aboriginal Community Controlled Health Organisations (ACCHOs),26,27 Australia lacks integrated community-based primary health services at scale,28 in particular those that offer specialist and mental health services delivered in a co-located hub. This is a significant barrier to states and territories implementing the NCAF.
At present, child protection case workers and families must navigate a complex, fragmented and under-resourced health system and long waiting lists, particularly for specialised trauma-focused services. This has led to inconsistencies in the level of health care that children receive – some might only have an initial visit with a GP, others might have a one-off assessment at a specialised assessment clinic for children in OoHC, while many might only receive care when they present with a crisis. Most never receive effective evidence-based treatment to ameliorate their trauma.
The current system is failing these children by not identifying their needs early and not providing targeted and evidence-based treatments delivered by specialised integrated services that wrap around the child and family. The NCAF states what children need, now a strategy is needed on how to deliver this successfully in Australia.


Image: Rob / Adobe Stock
Image: Rob / Adobe Stock
Health and wellbeing must be at the centre of child protection policy in Australia
Improving the health and wellbeing of children involved with the child protection system requires collaboration between the health and child protection systems. It also requires more explicit indicators within policy frameworks. For example, Safe and Supported: The National Framework for Protecting Australia’s Children 2021-203129 (NFPAC) presents an opportunity to address the gaps and inequities for Aboriginal children in OoHC. Developed together with Aboriginal and Torres Strait Islander people, it identifies Aboriginal children, those in OoHC, and those with complex needs as priority groups. The NFPAC embeds the four priority reforms of the National Agreement on Closing the Gap,30 including the urgent need to address the over-representation of Aboriginal children in the child protection system. The NFPAC’s first focus area is to develop a ‘national approach to early intervention and targeted support’ for vulnerable children, through developing multidisciplinary models, improving service navigation, and expanding evidence-based services, and in particular, improving services for Aboriginal children. However, the NFPAC does not reference the comprehensive guidelines for standardised health assessments in the National Clinical Assessment Framework, which was developed in 2011 for this very purpose. The NFPAC does not address the implementation difficulties and poor compliance with the NCAF health guidelines.
Similarly, the National Agreement on Closing the Gap’s target to reduce the rate of over-representation of Aboriginal children in OoHC by 45%, provides little emphasis on the role of health and wellbeing in achieving this goal. Health related indicators which might be used include the proportion of children who have completed comprehensive health checks on entry to care, the proportion of those identified with a disability, or measurement of those who have received trauma-informed psychological services.
Health care is important. Children with undiagnosed and untreated health, neurodevelopmental, and emotional problems often remain in the child protection system and may have trajectories into the criminal justice system.31 The lack of diagnosis and treatment can result in intergenerational involvement in both systems.
International lessons
During my Churchill Fellowship, I travelled to the USA, Canada and New Zealand to investigate how Australia could deliver standardised health care using a patient-centred integrated model of care for Aboriginal children in OoHC.32 The focus of my Churchill Fellowship was:
- to gain an in-depth understanding of patient-centred models of integrated care, including the ‘medical home’ or ‘health home’ model of integrated care
- to explore legislative reform which provides for accountable and equitable policies supporting the health care of Aboriginal children in care.
I found that firstly, the right type of health infrastructure is needed: specialised hubs offering integrated and co-located health (primary and specialist) and supportive services, and proportionate and equitable investment in culturally-safe hubs in Aboriginal community-controlled services. Secondly, legislative reform is needed to assign responsibility and ensure monitoring and reporting on the right health indicators to truly implement the NCAF.
Specialised models of integrated care for children in OoHC
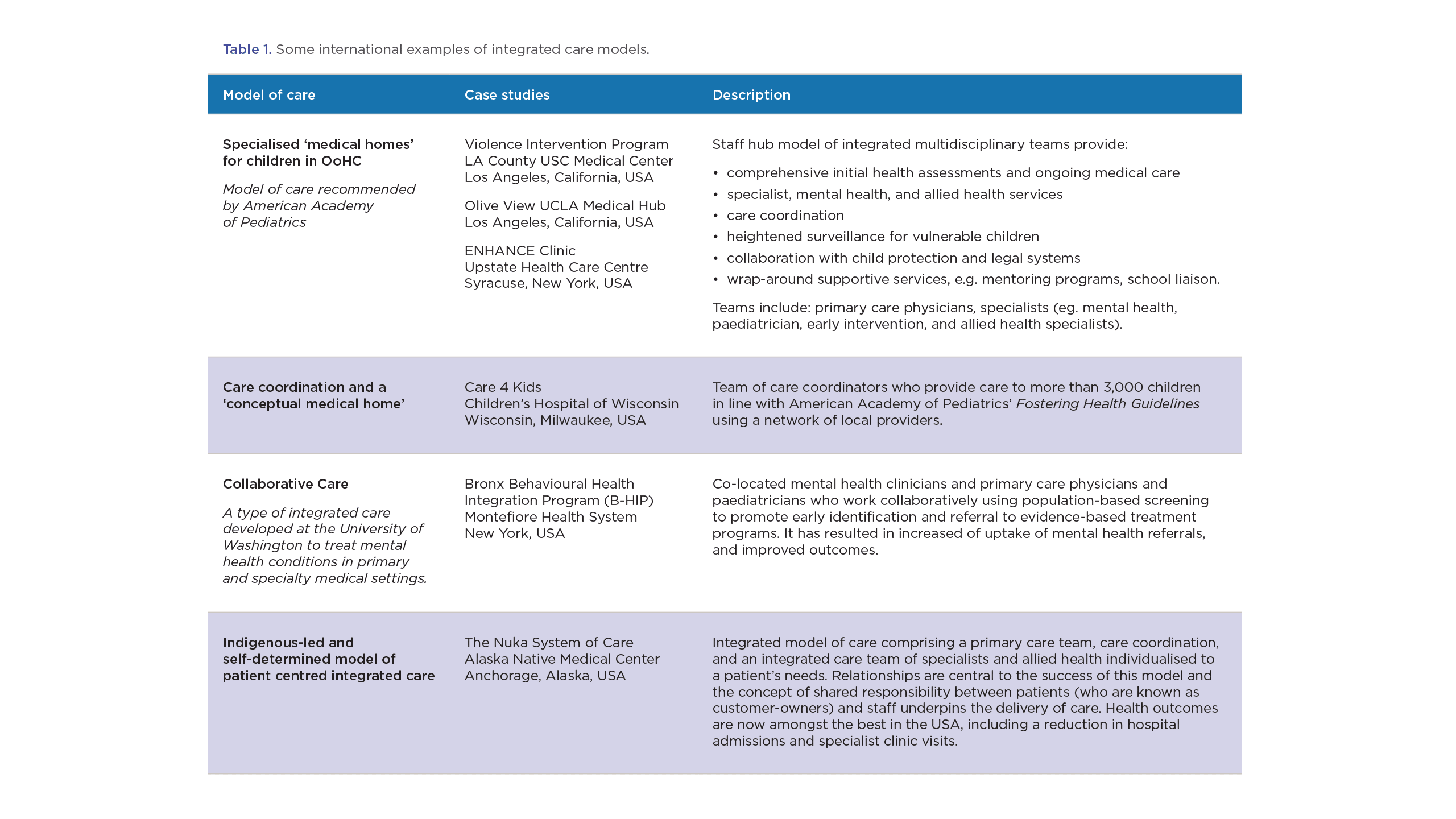
On my Churchill Fellowship, I investigated a range of specialised models of integrated care (Table 1). Integrated care is the name given to a type of health reform that seeks to deliver patient-centred and efficient care through a connected team of health care providers. The patient-centred medical home33 is one type of integrated care. I visited seven specialised medical home hubs for children in OoHC and other vulnerable children, as well as integrated care hubs for Indigenous populations, including the remarkable Nuka System of Care at the Alaska Native Health Center.34
In the USA, the American Academy of Pediatrics’ (AAP) standards of care for children in care, Fostering Health, recommends that health and preventative services are delivered through a medical home.35 I met with Professor Moira Szilagyi, President of the AAP, who led the taskforce that developed these guidelines. She told me that the rationale for this recommendation was that children in care have complex and special health needs, and need specialised, accessible, and intensive health services provided within a one-stop hub. A medical home ensures that care is coordinated, consistent, and trauma-informed, and proactive and preventative, rather than crisis-driven.
The medical homes I visited were one-stop hubs that provided primary and specialist medical care, mental health and social services, as well as care coordination and service navigation to not just children in OoHC, but other vulnerable children.
The Violence Intervention Project at the Los Angeles-University of Southern California Medical Center is LA County’s largest medical home hub for children in OoHC. It was founded by Dr Astrid Heger, an internationally renowned child abuse paediatrician. Its innovative service model provides integrated, wrap-around services to vulnerable children including a forensic clinic and community-based assessment and treatment in line with the AAP’s guidelines. The hub offers evidence-based mental health treatment programs, care coordination, parenting programs, a Foetal Alcohol Spectrum Disorder (FASD) assessment and treatment program, tutoring programs, allied health, school liaison and outreach programs, and social services. Dr Heger opined that to truly make a difference to vulnerable children, ‘it’s in the details’; they needed more than merely episodic medical care.
I visited ENHANCE Services for Children in Foster Care, in Syracuse, New York State, one of the longest running medical homes for children in OoHC in the USA. They have a specialised and skilled workforce who have built strong relationships with children and families they see. Biological parents often attend their children’s appointments, together with their foster carers, which aids in planning for reunification. Fragmented services can replicate the relational impermanence and trauma of a child’s early life. Trauma-informed and culturally-safe care is grounded in safe relationships, which is equally important in a child’s therapeutic team.
One of the most remarkable centres that I visited was the Indigenous-led Nuka System of Care at the Alaska Native Health Centre. It is renowned as one of the world’s leading models of health care redesign, and has transformed the health outcomes of its population. It has won numerous accolades including the USA Congress’ Malcolm Baldridge Award for quality in health care twice. Its model is a patient-centred medical home, which has radically reimagined health care delivery by prioritising equity, self-determination, and relationships. Care is delivered through a core primary care team that includes a care coordinator.
Care is individualised and coordinated through rigorous screening and stratification to specialist programs. They have achieved a range of improved health outcomes for their population, and have reduced health costs and emergency and hospital admissions. Cultural practices, wellbeing programs, and traditional healing is integrated into their programs.
Access to limited mental health services is a significant problem in Australia. Many of the hubs I visited used models of collaborative care (such as the Bronx B-HIP at the Montefiore Hospital). In this model, psychiatrists and psychologists worked in co-located medical clinics with paediatricians and primary care physicians, using robust screening and evidence based brief interventions to extend the reach of mental health services.36
The establishment of medical home hubs would assist the implementation of the NCAF, and would promote standardisation of care and address the fragmentation in the current system. While models of integrated care are not yet common in Australia, several trials and pilot programs are underway.37 ACCHOs have pioneered models of integrated care in Australia since the 1970s, offering community based primary care, with a range of wrap-around services. The self-determined ACCHO model needs to be recognised and sustainably funded.
Improving the health of Aboriginal children in OoHC and other vulnerable children will require Australian governments to invest in and develop specialised hubs or medical home models of integrated care in Aboriginal community-controlled health services and community hubs. They will align with the NCAF guidelines, offering patient-centred and strengths-based health, wellbeing, and supportive services.
Legislative reform
The USA has successfully enacted strong legislative reform to encourage the states to deliver health care to children in OoHC through a medical home, and has introduced reforms that require states to use evidence-based psychotherapeutic programs and monitor psychotropic medication use (Child and Family Services Improvement Innovation Act (2011).38 The Adoption and Safe Families Act (1997, ASFA) which reorientated the child welfare system towards permanency, resulted in a 27% decrease in children in care in the USA.39 The Family First Prevention Services Act (2018) goes further by releasing federal funds for early intervention and preventative programs to families of children at risk of entering care, including mental health services, substance abuse, and parenting programs, reorienting the child welfare system towards prevention and trauma-informed practice.40 To be funded, eligible therapeutic services need to meet evidence-based thresholds for effectiveness. The secretary of the Department of Health and Human Services publishes a list of evidence-based and approved services.
During my Churchill Fellowship, I met Mr Bryan Samuels, Commissioner of the Administration on Children, Youth and Families in the Obama Administration. Under his leadership, the USA Congress passed several pieces of legislation including the Fostering Connections to Success and Increasing Adoptions Act (2008) which strengthened the standards and oversight of the health of children in care. These reforms were strongly grounded in evidence-based and trauma-informed approaches, and an understanding of the cost-effectiveness of early intervention. Mr Samuels advised that beyond the crucial benchmarks of measuring safety and permanency, that health and wellbeing had to be the measuring stick for the performance of child welfare systems.
Strengthened legislative oversight combined with targeted and proportionate investment in ACCHOs will help vulnerable Aboriginal children access comprehensive multidisciplinary care. This is crucial in helping them to thrive and shifting their life trajectories.
Stakeholder consultation
My application for a Churchill Fellowship developed from conversations that I had with Mr Andrew Jackomos PSM, inaugural Commissioner for Aboriginal Children and Young People in Victoria, following my participation in the Taskforce 1000 Inquiry, which examined many of the unmet needs of Aboriginal children in state care in Victoria. Mr Jackomos, who was one of my referees, has remained a steady source of counsel and support as I developed my report and recommendations, and disseminated my work. Ms Nicole McCartney, Victorian Department of Health’s Chief Aboriginal Health Advisor, who is my policy peer reviewer, has provided invaluable guidance on this paper. I have consulted with Ms Jill Gallagher AO, CEO of VACCHO, and Mr Michael Graham, CEO of the Victorian Aboriginal Health Service, who have both supported my recommendations.
My work has informed policy and advocacy work at the Royal Australasian College of Physicians, where I have been a contributing author to policy papers on the health of Indigenous children, and the health of children in care and protective services. Many of my recommendations have been incorporated into RACP policy documents.
My Churchill Fellowship report has been provided to a range of stakeholders including Safer Care Victoria, the Consultative Council for Obstetric and Paediatric Mortality and Morbidity, State Minister for Health, and department secretaries.
Consultations have been sought with other Aboriginal peak bodies including NACCHO, VACCA, and SNAICC.
Policy recommendations
1. The Australian Government should develop a national health and wellbeing action plan for children in out-of-home care to accompany Safe and Supported: The National Framework for Protecting Australia’s Children 2021-2031. This will be a roadmap to implement the National Clinical Assessment Framework for Children and Young People in Out-of-home Care (2011).41 The Plan should be co-designed with the Aboriginal community-controlled sector.
The Plan should:
- mandate health assessments for every child in OoHC in line with the NCAF
- clarify the statutory responsibility, funding, and resourcing for health care
- include a robust statutory and regulatory framework that includes national health indicators to measure and report on the health and wellbeing of children in the child protection system, including those in out-of-home care and specifically address the health of Aboriginal children in care, aligning with the socio-economic targets in the National Agreement on Closing the Gap (2020).42
2. The Australian Government should invest in and develop specialised multidisciplinary Integrated Care hubs for vulnerable children, including those in out-of-home care, ACCHOs, and community hubs, to deliver integrated, culturally safe, and trauma-informed primary health, specialist, mental health, and supportive care.
Acknowledgements
I acknowledge and thank my policy peer reviewers: Nicole McCartney, Chief Aboriginal Health Advisor, Victorian Department of Health, Dr Susan Webster, Honorary Research Fellow, University of Melbourne Medical School, and Associate Professor Susan Woolfenden, School of Public Health, University of Sydney, for their generous advice and insights. I am very grateful to Magistrate Jennifer Bowles, Churchill Fellow, for her insights, advice and encouragement.
Published 30 November 2022


Dr Niroshini Kennedy is a Paediatrician at the Victorian Aboriginal Health Service. Her policy and advocacy work is informed by her clinical work with Aboriginal children in the child protection and OoHC systems. She is President-Elect of the Paediatric Division of the Royal Australasian College of Physicians and a member of Victoria's Consultative Council on Obstetric and Paediatric Mortality and Morbidity. Read more about Niroshini Kennedy and her Churchill Fellowship.
References and endnotes
- An Aboriginal Community Controlled Health Organisation (ACCHO) is a primary health care service initiated, operated, and governed by the local Aboriginal community.
- The term Aboriginal in this paper refers to both Aboriginal and Torres Strait Islander People. The term Indigenous is retained when it has been used as part of a quotation, or the title of a program or report, or used in an international context. This is consistent with the nomenclature endorsed by NACCHO (National Aboriginal Community Controlled Health Organisation).
- The AIHW defines out-of-home care (OoHC) as ‘alternative accommodation for children under 18 years who are unable to live with their parents, where the State or Territory makes a financial payment, or where a financial payment has been offered but declined’. Most of these children will be subject to statutory child protection orders and may be in kinship, foster or residential care.
Australian Institute of Health and Welfare (AIHW). ‘Australia's children’. AIHW, Accessed 9 June 2022.
AIHW. Child protection Australia 2019–20, Canberra: AIHW, Australian Government. 18 May 2021.
https://doi.org/10.25816/g208-rp81
SNAICC. The Family Matters Report 2021. Eltham: Postscript Printing and Publishing, 2021. https://www.familymatters.org.au/the-family-matters-report-2021/
Szilagyi, M, Rosen, D, Rubin, D, and Zlotnik, S. ‘Health care issues for children and adolescents in foster care and kinship care.’ Pediatrics, 136, 4 (2015).
https://doi.org/10.1542 peds.2015-2656
Nathanson, D, and Tzioumi, D. ‘Health needs of Australian children living in out-of-home care.’ Journal of Paediatrics and Child Health, 43 (2007), 695–699. https://doi.org/10.1111/j.1440-1754.2007.01193.x
Kennedy, N. Improving the Health of Aboriginal Children in Out-of-Home Care: The 2018 Jack Brockhoff Foundation Churchill Fellowship to investigate integrated models of care for Aboriginal children in out-of-home care. Churchill Fellowship Report: The Winston Churchill Memorial Trust, 2020. https://www.churchilltrust.com.au/project/the-jack-brockhoff-foundation-churchill-fellowship-to-investigate-integrated-models-of-care-for-aboriginal-children-in-out-of-home-care/
Commission for Children and Young People. Always was, always will be Koori Children: Systemic inquiry into services provided to Aboriginal children and young people in out-of-home care in Victoria. Melbourne: Commission for Children and Young People, 2001.
Raman S, Reynolds, S, and Khan, R. ‘Addressing the wellbeing of Aboriginal children in out-of-home care: are we there yet?’ Journal of Paediatrics and Child Health, 47, 11 (2011), 806-11.
Shmerling, E, Creati, M, Belfrage, M, and Hedges, S. ‘The health needs of Aboriginal and Torres Strait Islander children in out-of-home care.’ Journal of Paediatrics and Child Health, 56, 3 (2020).
https://doi.org/10.1111/jpc.14624
McLean, K, Little, K, Hiscock, H, Scott, D, and Goldfeld, S. ‘Health needs and timeliness of assessment of Victorian children entering out-of-home care: An audit of a multidisciplinary assessment clinic.’ Journal of Paediatrics and Child Health, 55, 12 (2019), 1470-1475. https://doi.org/10.1111/jpc.14472
Teager, W, Stacey, F, and Neil, S. How Australia can invest early and return more: A new look at the $15b cost and opportunity. Australia: Early Intervention Foundation, The Front Project and Telethon Kids Institute, 2019.
Commission for Children and Young People. Our youth, our way: inquiry into the overrepresentation of Aboriginal children and young people in the Victorian youth justice system, Summary and recommendations, Melbourne: Commission for Children and Young People, 2021.
NSW Government. Their Futures Matter: A New Approach, The intergenerational cycle of abuse and neglect, 2018. https://www. childabuseroyalcommission.gov.au/sites/default/files/WEB.0189.001.1036.pdf
AIHW. ‘Income support receipt for young people transitioning from out-of-home care’. Accessed July 2022. https://www.aihw.gov.au/reports/ child-protection/incomesupport-receipt-oohc/summary
Department of Health. National Clinical Assessment Framework for children and young people in out-of-home care. Canberra: Australian Government, 2011. http://health.gov.au/internet/publications/publishing.nsf/Content/ncaf-cyp-oohc-toc
Royal Australasian College of Physicians (RACP). Health of children in ‘out-of-home’ care. Sydney: RACP, 2006. https://www.racp.edu.au/docs/default-source/advocacy-library/health-of-children-in-out-of-home-care.pdf
Royal Australian and New Zealand College of Psychiatrists (RANZCP). ‘Position statement: The mental health care needs of children in out-of-home care.’ RANZCP, March 2015. https://www.ranzcp.org/news-policy/policy-and-advocacy/position-statements/the-mental-health-needs-of-children-in-care
ACIL Allen Consulting. Health Assessments and Interventions for children and young people in the child protection system: Options Paper to Department of Social Services. Melbourne: ACIL Allen Consulting, 2013.
McLean, K, Hiscock, H, and Goldfeld, S. ‘Timeliness and extent of health service use by Victorian (Australian) children within first year after entry to out-of-home care: Retrospective data linkage cohort study.’ Children and Youth Services Review. 1, 134 (2022), 106359. https://doi.org/10.1016/j.childyouth.2021.106359
ACIL, Health Assessments and Interventions.
Department of Families, Housing, Community Services and Indigenous Affairs and the National Framework Implementation Working Group. National Standards for Out-of-Home Care. Canberra: Commonwealth of Australia, 2011. https://www.dss.gov.au/sites/default/files/documents/pac_national_standard.pdf
Webster, S. Children and young people in statutory out-of-home care: health needs and health care in the 21st century. Victoria: Parliamentary Library and Information Service, 2016.
Panaretto, K, Mark, W, Selwyn, B, and Ian, T. ‘Aboriginal community controlled health services: leading the way in primary care.’ Medical Journal of Australia 200, 11 (2014), 649-652. https://doi.org/10.5694/mja13.00005
Pearson, O, Schwartzkopff, K, Dawson, A, Hagger, C, Karagi, A, Davy, C, Brown, A, and Braunack-Mayer, A. ‘Aboriginal community controlled health organisations address health equity through action on the social determinants of health of Aboriginal and Torres Strait Islander peoples in Australia.’ BMC Public Health, 20, 1 (2020), 1-13. https://doi.org/10.1186/s12889-020-09943-4
Royal Australasian College of Physicians (RACP). Integrated Care: Physicians supporting better patient outcomes. A discussion paper. Canberra: RACP, 2018.
Department of Social Services. ‘Safe and Supported: the National Framework for Protecting Australia’s Children 2021–2031’. Accessed July 2022. https://www.dss.gov.au/our-responsibilities/families-and-children/programs-services/protecting-australias-children
Joint Council on Closing the Gap. ‘National Agreement on Closing the Gap’. Accessed July 2022. https://www.closingthegap.gov.au/national-agreement
Bower, C, Watkins, R, Mutch, R, Marriott, R, Freeman, J, Kippin, N, Safe, B, Pestell, C, Cheung, C, Shield, H, and Tarratt, L. ‘Foetal alcohol spectrum disorder and youth justice: a prevalence study among young people sentenced to detention in Western Australia.’ BMJ open, 8, 2 (2018), 019605. https://doi.org/10.1136/bmjopen-2017-019605
Kennedy, Improving the Health of Aboriginal Children
Also known as a ‘Patient-centred Medical Home,’ this is a form of integrated care that is characterised by team-based care delivery, with care coordination, that aims to provide continuous and comprehensive care.
Gottlieb, K. ‘The Nuka System of Care: improving health through ownership and relationships.’ International journal of circumpolar health, 72 (2013). https://doi.org/10.3402/ijch.v72i0.21118
Task Force on Health Care for Children in Foster Care, Fostering Health: Health Care for Children and Adolescents in Foster Care, 2nd Edition. USA: American Academy of Pediatrics, 2005.
Germán, M, Rinke, M, Gurney, B, Gross, R, Bloomfield, D, Haliczer, L, Colman, S, Racine, A, and Briggs, R. ‘Comparing two models of integrated behavioral health programs in pediatric primary care.’ Child and Adolescent Psychiatric Clinics, 26, 4 (2017), 815-828.
Department of Human Services. ‘Australian Health Care Homes Trial’. Accessed July 2022,
https://www.humanservices.gov.au/organisations/health-professionals/subjects/health-care-homes
‘Bryan Samuels on Psychotropics and Foster Care.’ Administration for Children and Families, 1 December 2011. https://www.acf.hhs.gov/archive/testimony/bryan-samuels-psychotropics-and-foster-care
‘Trends in Foster Care and Adoption.’ Administration on Children, Youth and Families, 30 November 2021. https://www.acf.hhs.gov/cb/resource/trends-in-foster-care-and-adoption
Child Welfare Information Gateway. Health-care coverage for children and youth in foster care—and after. US: Children's Bureau, 2022. https://www.childwelfare.gov/pubs/issue-briefs/health-care-foster/
Kennedy, ‘Improving the Health of Aboriginal Children’.
Closing the Gap, ‘National Agreement’.
Key terms: First Nations, out-of-home care, Aboriginal children, integrated care, medical home, child protection
